
High blood pressure is a chronic condition that can have multiple causes. Among them, the increase in a hormone, aldosterone, produced by the adrenal glands located above the kidneys. And this form of hypertension has the double defect of being more difficult to diagnose and more difficult to treat. But a discovery could change the situation.
A quick exam to visualize the adrenals
Researchers from University College London (UCL) have developed a new scanner, capable of transforming the care of millions of patients suffering from hypertension. Indeed, this rapid examination reveals overactivity of the adrenal glands invisible to conventional tests, making it possible to direct treatments more precisely.
The main challenge of this examination is therefore to better diagnose primary hyperaldosteronism, a common but underestimated cause of resistant hypertension. For researchers, the simplicity and precision of this technique could alleviate a diagnostic process that is currently long and invasive.
A scan that visualizes the disease for the first time
But how does it work? The device developed at UCL, presented in the New England Journal of Medicine,
uses a radioactive tracer detected by the Pet-scan. It helps locate adrenal areas that produce too much aldosterone.
“The tracer targeting aldosterone synthase (CYP11B2) can precisely identify areas of the adrenal glands that excessively produce aldosterone. It thus becomes a valuable tool for diagnosing primary hyperaldosteronism, responsible for 5 to 10% of resistant arterial hypertension.” first describes Dr. Gérald Kierzek, emergency physician and medical director of True Medical.
The first uses of the scanner made it possible to precisely locate areas of overproduction in 17 patients, without any side effects. Professor Bryan Williams, chair of the Department of Medicine at UCL and leader of the study, summarizes the visual impact of the technique.
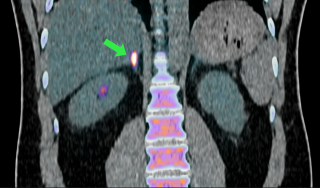
“This is the first time we can visualize this disease. You can see it light up on the scan. The intensity of the signal reflects the level of aldosterone overproduction. This could allow us, in the future, to target these overproducing areas more precisely.”
 © UCL
© UCL
Imaging showing hyperaldosteronemia
A common disease but difficult to identify
Hyperaldosteronism remains too often overlooked despite its major role in resistant hypertension. “Primary hyperaldosteronism corresponds to an autonomous secretion of aldosterone by the adrenals. In approximately 60% of cases, it is a Conn adenoma; in 30%, a bilateral hyperplasia” adds Dr. Kierzek.
“This hormone increases sodium retention, promotes potassium elimination – which can lead to hypokalemia – and causes vasoconstriction. The result is severe hypertension, often associated with cardiovascular complications, even though renin (another hormone) is suppressed.”
An exam that replaces a cumbersome procedure
Today, diagnosis follows a demanding multi-step process.
“Diagnosis is initially based on screening showing an elevated aldosterone/renin ratio (usually greater than 20–30) in patients with resistant hypertension or spontaneous hypokalemia. he says again.
“Confirmation is done by a suppression test (saline or captopril), followed by a CT scan or MRI of the adrenals. The current reference remains bilateral catheterization of the adrenal veins, an invasive examination but successful in more than 90% of cases, making it possible to distinguish unilateral damage from bilateral damage.“.
In summary, the diagnosis is based on a blood test, confirmed by a second test. To determine the treatment, two catheters are inserted into veins on either side of the groin to measure the aldosterone level on each side of the body. This allows doctors to determine whether the problem is with just one adrenal gland or both. However, this test is not always reliable and is rarely offered, as few hospitals have the expertise to perform this complex procedure.
This new scanner could therefore limit the use of this cumbersome, poorly available and sometimes imprecise procedure.
“We have been waiting for a test like this for many decades. This British innovation will transform the diagnosis of excess aldosterone into an important and previously hidden cause of hypertension in many of our patients. It offers enormous potential to completely change the way we make this diagnosis and allow us to offer better targeted treatment to our patients.” welcomes Professor Bryan Williams.
Towards better targeted treatments
Finally, the therapeutic choice is refined, thanks to this examination and depends on the location of the overproduction of aldosterone. According to our expert,
- Treatment can be surgical, with laparoscopic adrenectomy in cases of unilateral adenoma, making it possible to cure hypertension in 50 to 70% of cases and to normalize serum potassium;
- It can also be medical, based on aldosterone antagonists such as spironolactone (50–100 mg/day, up to 300–400 mg) or eplerenone, particularly for bilateral hyperplasia or non-operable patients; amiloride can be added if necessary.
A new technique to simplify the treatment strategy
“This new non-invasive scan, specifically targeting CYP11B2, clearly highlights hyperproducing nodules, without the ambiguities of traditional CT scans or MRIs whose specificity remains limited. It could, for many patients, replace adrenal catheterization, simplifying the diagnostic pathway, avoiding unnecessary interventions and accelerating access to treatment, whether surgical or medical. Wide adoption would reduce costs, risks and delays, while making diagnosis more accessible in everyday practice” analyzes Dr. Kierzek again.
Our expert, however, points out an essential limit. “However, it should be remembered that this system only concerns a minority of cases of high blood pressure.
A point which does not prevent Professor Erik Arstad, who co-developed this tracer after more than ten years of research, from welcoming this milestone.
“It is very rewarding to be able to bring laboratory innovation into the clinic to benefit patients with difficult-to-treat hypertension.”
The team is currently conducting a phase 2 clinical trial to gather sufficient data for possible approval of the review by the English health system.